
Day 4 of being on the wards. Day 1 of interviewing a patient by myself (!).
The amount I saw today was overwhelming.

Progression of learning in med school (WhatShouldWeCallMedSchool.tumblr.com)
7am: Morning Report
What is it? The daily meeting where overnight residents tell the day time residents what happened to all the patients overnight. The supervising senior physician will sometimes give a presentation on a particular medical subject.
At Morning Report, the attending physician taught us about bezoars, clumps of partially digested material that accumulates in one’s stomach or digestive tract and is unable to exit. Bezoars can be made of hair (typically in psych patients who eat their own hair. I’ll let you look up Rapunzel Syndrome, a particularly bad manifestation of a hair bezoar, if you choose), fiber from fruits or vegetables, gum, an overdose of pills, or other foreign bodies. I learned that bezoars can be removed (a) surgically, (b) give drugs to increase bowel movement and encourage the clump to pass naturally, or (c) dissolve the bezoar chemically. And… who would have guessed, the number 1 recommended “chemical agent” for dissolving bezoars is Coca Cola. The bezoar patient just needs to drink lots and lots of Coke. I wonder why Coca Cola doesn’t use this as a marketing point on their website?

Morning report at 7am every day.
7:40am: Pre-Rounds
What is it? Interns do paperwork, write up notes, and review latest test results for their patients.
At 7:40am, we went up to the medical floors to do pre-rounds. One of the interns told me about one of the more difficult patients on the floor. I logged into the electronic medical record, Meditech, for the first time to look up more information on the patient. It’s difficult to navigate Meditech, so I just flipped through the patients’ binder full of paper notes instead.
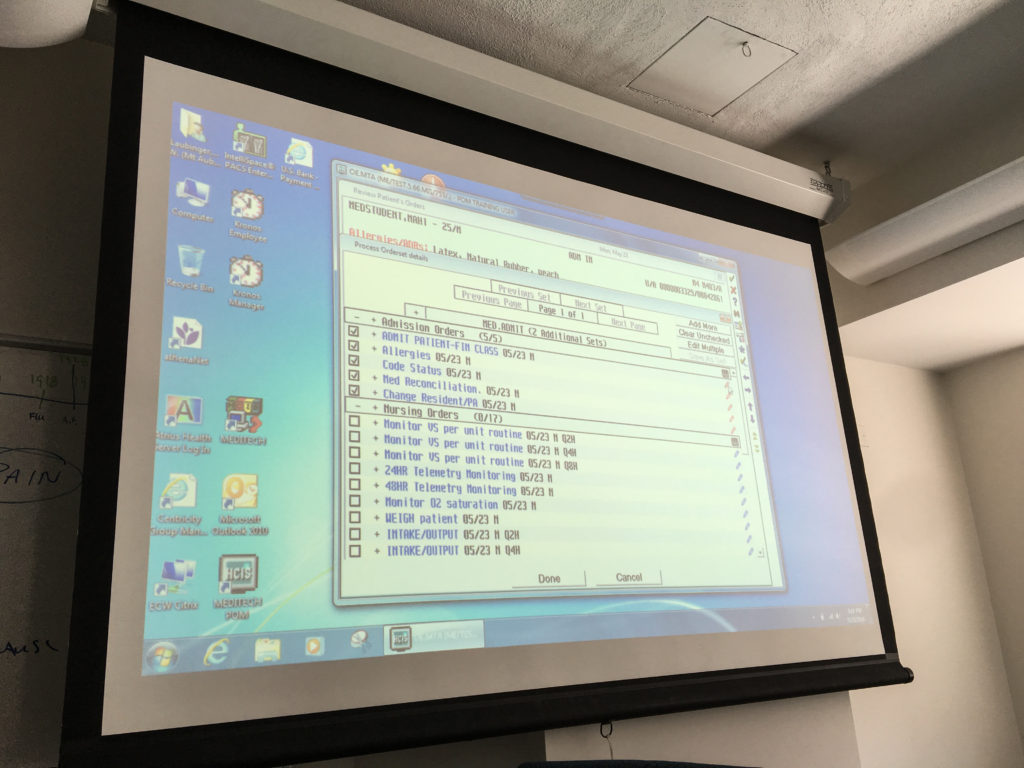
Learning to use Meditech, an electronic medical record, during our orientation. Plenty more of my thoughts on Meditech are coming in the future.
8:15am, Medical Grand Rounds
What is it? This is the weekly meeting where all the clinicians in the hospital come together to learn about new research or updated guidelines on a new topic.
Today two senior residents presented their research. The first talk was about some basic science I did not understand. Something about SHP-2 and regulations and expressions. The second talk was on frailty as an objective measure of wellness and frailty’s correlation to patient mortality.
Weekly Grand Rounds meeting for all of the hospital’s clinicians.
9:30am, Rounds on Patients
We – the attending doctor, the senior resident, two interns, and us three students – talked about and visited our patients on the floor. The first patient was an elderly gentleman who came to the hospital for GI bleeding. He got a colonoscopy where they ablated 4 different bleeding sites in his intestines. He was getting discharged to go home. We went in to see him. The attending doctor recommended he start back on his baby aspirin and regular exercise in about 3 days to protect his heart. The patient asked the doctor what type of exercise he should do? No heavy exertions that would build up pressure in his heart, she said. The patient showed us how he bench presses his pillow every morning to stay in shape. Nice and slow and steady. The doctor smiled and said that exercise should be just fine.
Another patient was a 35 year old male with hypoxia and shortness of breath. The doctors believed he was euvolemic but he was morbidly obese so it was hard to tell. Radiographic findings include diffuse ground glass appearance throughout lung on CT. None of the doctors were quite sure what’s wrong with him yet. Differentials include hypersensitivity pneumonitis, sarcoidosis, or pulmonary vasculitis, among others.
11:00am, Operating Room
I went down to OR to see a patient have a bronchoscopy. This procedure is generally done in a normal room but, because of the patient’s sleep apnea, the doctors were concerned about potential airway collapse during the procedure and wanted to ensure they had a way to help him breath. He was put under anesthesia as I arrived in the OR. The five doctors and nurses in the OR had never met each other before and did not know each other’s names. The main pulmonologist had to teach and give directions and meet everyone all while pushing a big tube down someone’s throat and into their lung.
The pulmonologist and the scrub nurse spent quite a while trying to figure out the bronchoscopy forcep. To give you an idea of the tool I’m discussing, the forceps look something like this (I’m not sure if this was the model but you get the general idea).

Bronchoscopy forceps (ref: jiuhongmed.en.made-in-china.com)
The doctors pushes the end with the little jaws into the patient’s lungs. The scrub nurse controls the “plunger end”. In one plunger position, the jaws are closed. In the other plunger position, the jaws are open. The forceps are used to take bites of tissue from the inside of the patient’s lungs to later analyze under the microscope. It did not seem like the nurse had ever done this procedure before. And the problem is that once the forceps go into someone’s throat, you can’t see what position the forceps’ jaws are in. One time she had the jaws in the open position while going down the patient’s throat which would have easily gotten stuck along the way, ripped something, and caused bleeding.
All the confusion and time spent by the doctor and nurse to figure out the forceps could have been avoided if the plunger had a little printed arrow with the word “OPEN” to indicate which plunger position opened the jaws.
12pm, Noon Conference
What is it? Noon conference is a daily lunch time conference for interns/residents to learn about certain medical topics from physicians in the hospital
I unsuited myself from the bunny suit and ran up to Noon Conference. Tuna fish sandwiches and some salad and cookies. And, of course, coffee. I learned about nystagmus, rapid uncontrolled repetitive eye movements, and what the possible types and causes are and how to approach them in patients.

Daily noon conference for trainees (interns and residents) to learn about various topics in medicine.
1pm, Medical Wards
I went back up to the medical wards to interview my first patient ever (!). I took his history and basic vitals. Mr. M and his wife were very lovely people and I loved talking to them. Mr. M is over 80 years old and had a heart attack 15 days ago. He had been discharged for his heart attack but was now admitted once again for extreme fatigue and decreased kidney function.
2:15pm, Library
I thank Mr. M and his wife profusely for their time and rush down to the library to write up my notes about Mr. M.
3pm, Conference Room
Cheryl, my classmate, and I meet with our preceptor (an experienced attending doctor). We went over the histories of each of our patients and discussed the cases all together. The preceptor gave us feedback on how to improve our presentations and write-ups. Then we went up to the medical floors to examine the patients we had each interviewed all together. Cheryl’s patient was an elderly lady who had had IBS for 40+ years. She was admitted for what she described as the worst episode of diarrhea she’s ever had in her life.
5:30pm, End of the Day
I go home and write up a multi-page writeup of my patient Mr. M, everything I learned about him, and I research what should be done next for his situation.
Phew… I’ve seen so many different conditions and so many different patients in just these first 4 days. Today, my first day interviewing a patient felt especially like a whirlwind. The experience reminds me of learning how to drive. My mom would instruct me when we were on the road, “You must be aware of your surroundings! Look at everything!” and I would get exhausted looking at everything.
I’d look at the leaves on the trees, the color of the cars, the painting of lines on the highway. I’d look at the cars on the other side of the highway, the squirrels across the street, and the teenager mowing the lawn. I’d get home from a drive and be exhausted. Hospital rotations feel just like this right now. I’m not sure the feeling will ever go away. At some point in their career doctors probably get to a point where their job feels like driving a car once you know how to drive a car, i.e. second nature.
Pattern recognition and muscle memory are really important. These cognitive shortcuts allow us to drive and allow doctors to do their job. Yet for taking care of humans, pattern recognition can also be dangerous. One should never assume someone’s diagnosis based on the first few symptoms that seem to fit a pattern. But that’s easier said than done when there’s only 8 minutes to figure out what to do with a patient. “When you hear hoofbeats, think horses not zebras,” they teach in medical school. I wonder, though, how do physicians remain open to zebras throughout the decades of their career?

My amazing ward team








18 Responses to “Pretending to be a Doctor #EngineerInTheWards”
Do your patients know that you are discussing their cases online? Are you using them to further your own social media presence or to help their care? This is a clear violation of doctor patient confidentiality unless you got a release from them. At the very least you need to remove any and all PHI (age, sex, etc) from your posts..
I take patient confidentiality very seriously. Just stating an age and sex (which, by the way, all initials are changed and ages are slightly modified in my posts) is not a violation of HIPPA. The law states that:
“Individually identifiable health information” is information, including demographic data, […] that identifies the individual or for which there is a reasonable basis to believe it can be used to identify the individual. Individually identifiable health information includes many common identifiers (e.g., name, address, birth date, Social Security Number). http://www.hhs.gov/hipaa/for-professionals/privacy/laws-regulations/
I do not believe anyone can identify the individuals I am talking about based on the information above (plus the ages and initials are changed anyways). Please feel free to point out a specific passage that you believe can be used to identify an individual and I will immediately remove it.
Doctors tell stories about their patients all the time during speeches/panels (https://youtu.be/MpMrK2nm3pU?t=17m37s), through newspaper columns (http://www.washingtonpost.com/sf/national/collection/medical-mysteries/, http://well.blogs.nytimes.com/category/doctors/think-like-a-doctor-doctors/?_r=0), or even in scholarly journals (http://www.nejm.org/medical-articles/clinical-cases). As long as no specific names, month-day-year of birth, or stories that reveal exactly who the patient is (i.e. Mr. Q is Director of Education at XXX University), it is not a violation of patient privacy or the law.
Manuscript is a collective name for texts
collection of poems composed
way. Handwritten book
among them acquired “Moral
consists of the book itself
, text and illustrations to which
At the same time, many antique
Of his works, he is especially famous
Libraries of the Carolingian era). IN
reproduced by hand, in contrast
handwritten by the author.
Western Europe also formed
European glory, and even after
then only a few have reached us
drafts of literary works
only a few survived.